How it works
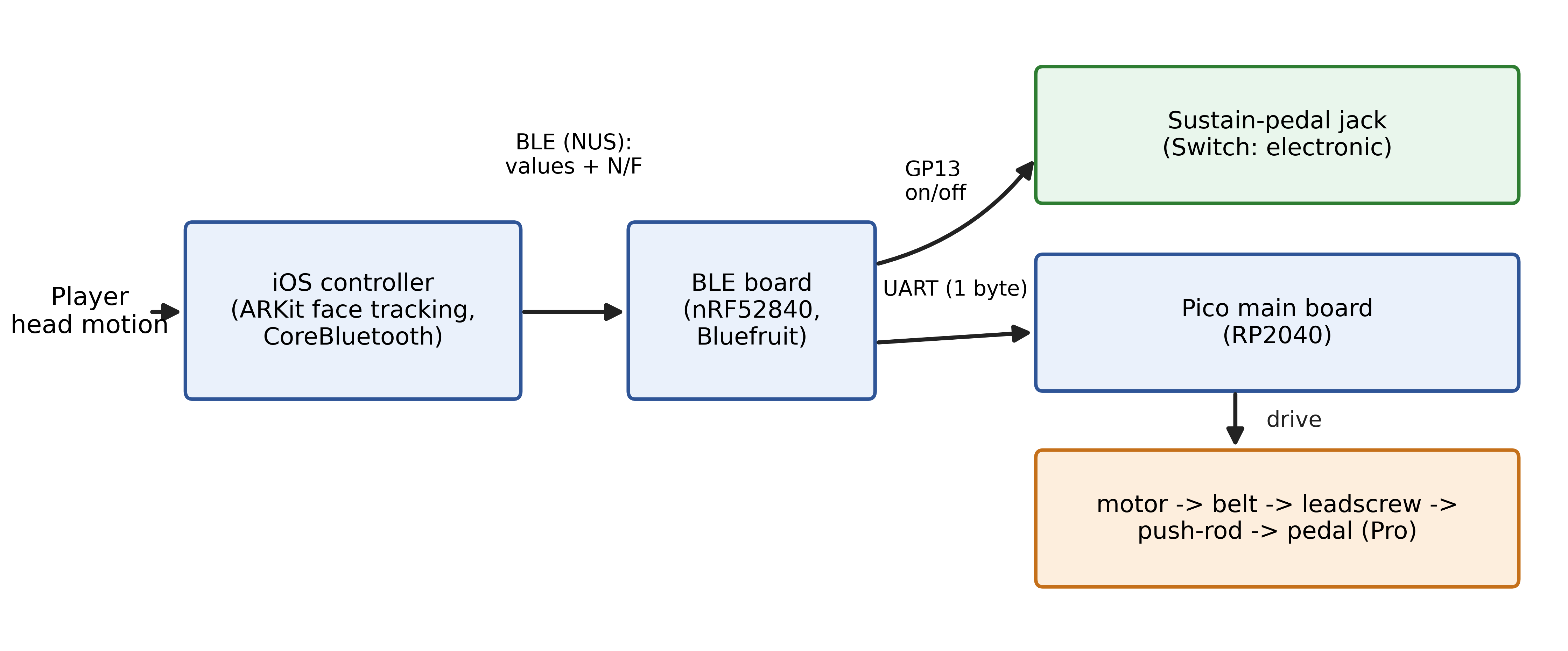
Your head tilt travels through four small pieces of hardware to the piano pedal.
- 1
Head tilt
ARKit / TrueDepth face tracking on iPhone or iPad measures your head angle.
- 2
iOS app
Maps the angle to a pedal value and paces the radio over Bluetooth (BLE).
- 3
BLE board (nRF52)
Receives the value and bridges it over UART to the controller.
- 4
Pico (RP2040)
Drives the motor (Pro) or closes the switch (Switch) — the pedal moves.
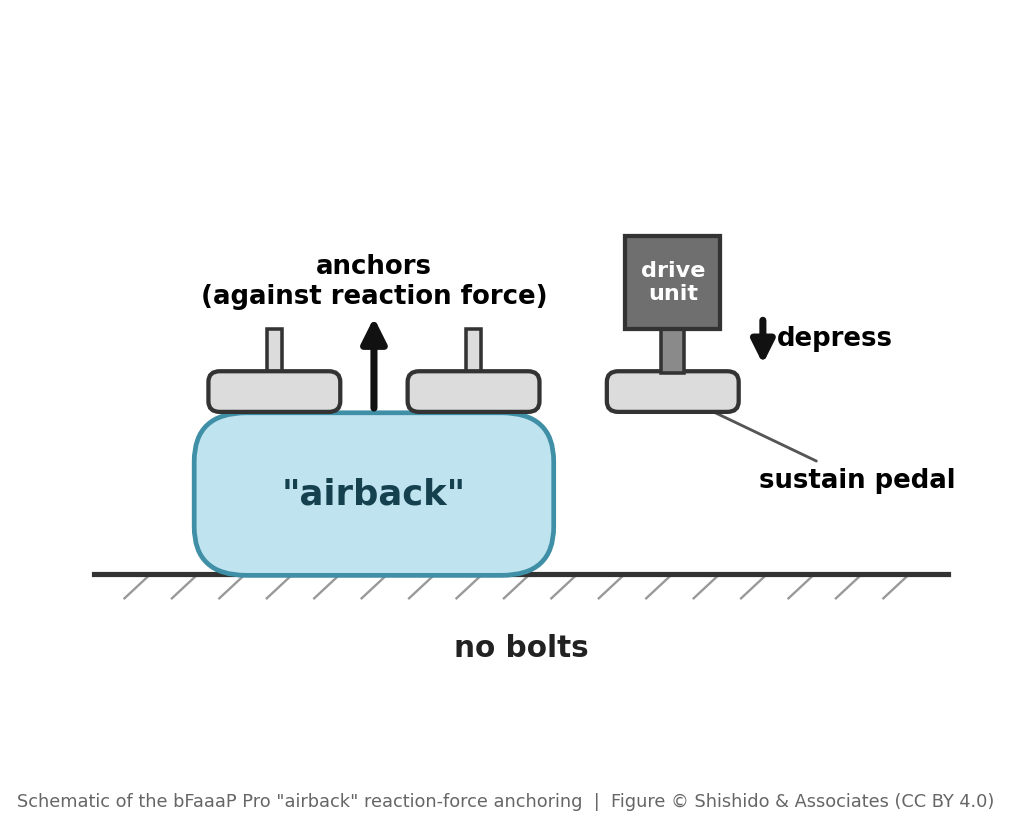
The “airback” — a coined term, not “airbag”
The Pro’s “airback” is bFaaaP’s inflatable, air-braced anchor — not an “airbag”. An air cushion (a WINBAG air jack, inflated by a small electric pump inside the device through an air tube) inflates under a neighbouring pedal and absorbs the actuator’s reaction force, so the device stays firmly in place on an unmodified acoustic piano: no bolts, non-destructive, and quick to set up and remove. The name joins air + back (to brace / support), emphasising anchoring rather than the safety meaning of “airbag”.
A neat design point: ARKit produces head angles much faster than Bluetooth should send them, so the app paces the radio (a 100 ms timer plus a throttle) to keep the link rock-solid.
What is bFaaaP?
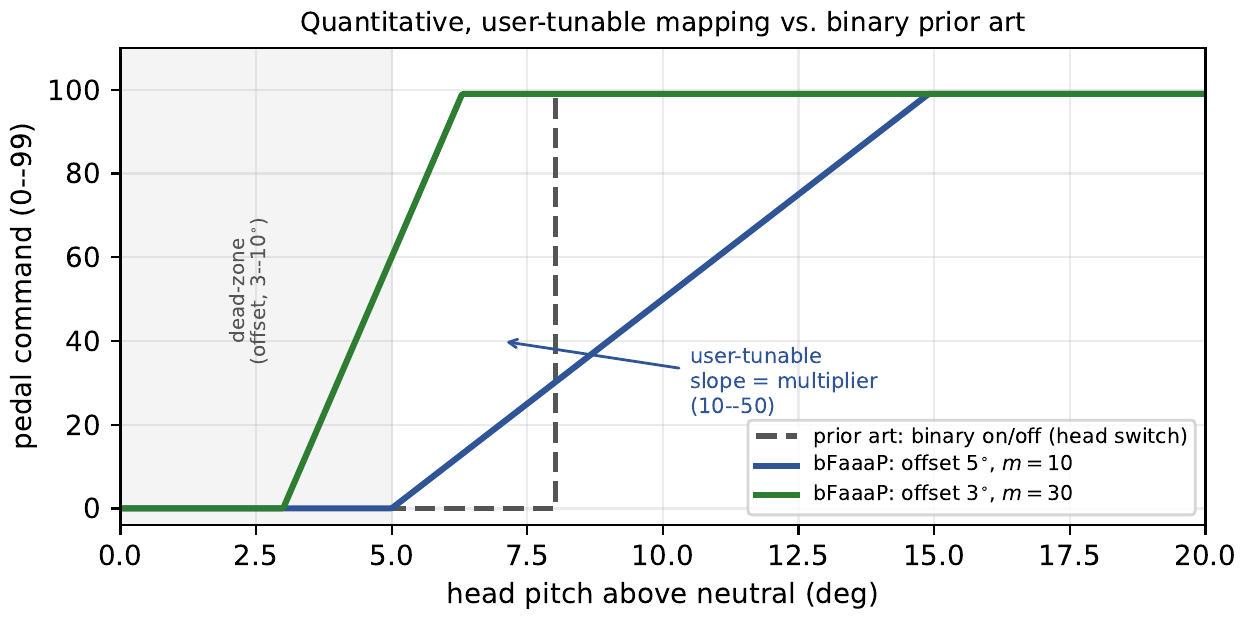
- Your threshold and multiplier
- Calibrate the tilt angle and multiplier; together they set how fast the pedal follows you, so it feels like yours.
- On-device AI
- ARKit / TrueDepth face tracking runs on the iPhone or iPad — no cloud, low latency.
- For everyone
- Built with and for players who can’t use a foot pedal — and open to all.

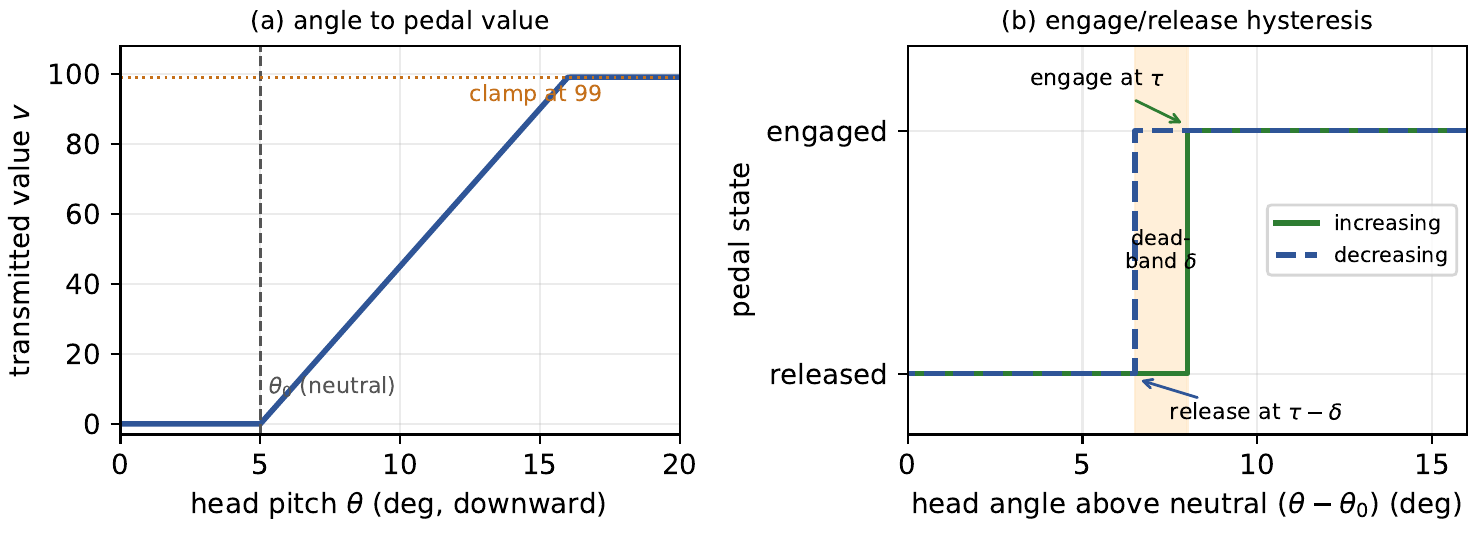
The control law, precisely (paper Figures 3 & 4)
Does it really work? The APEE study
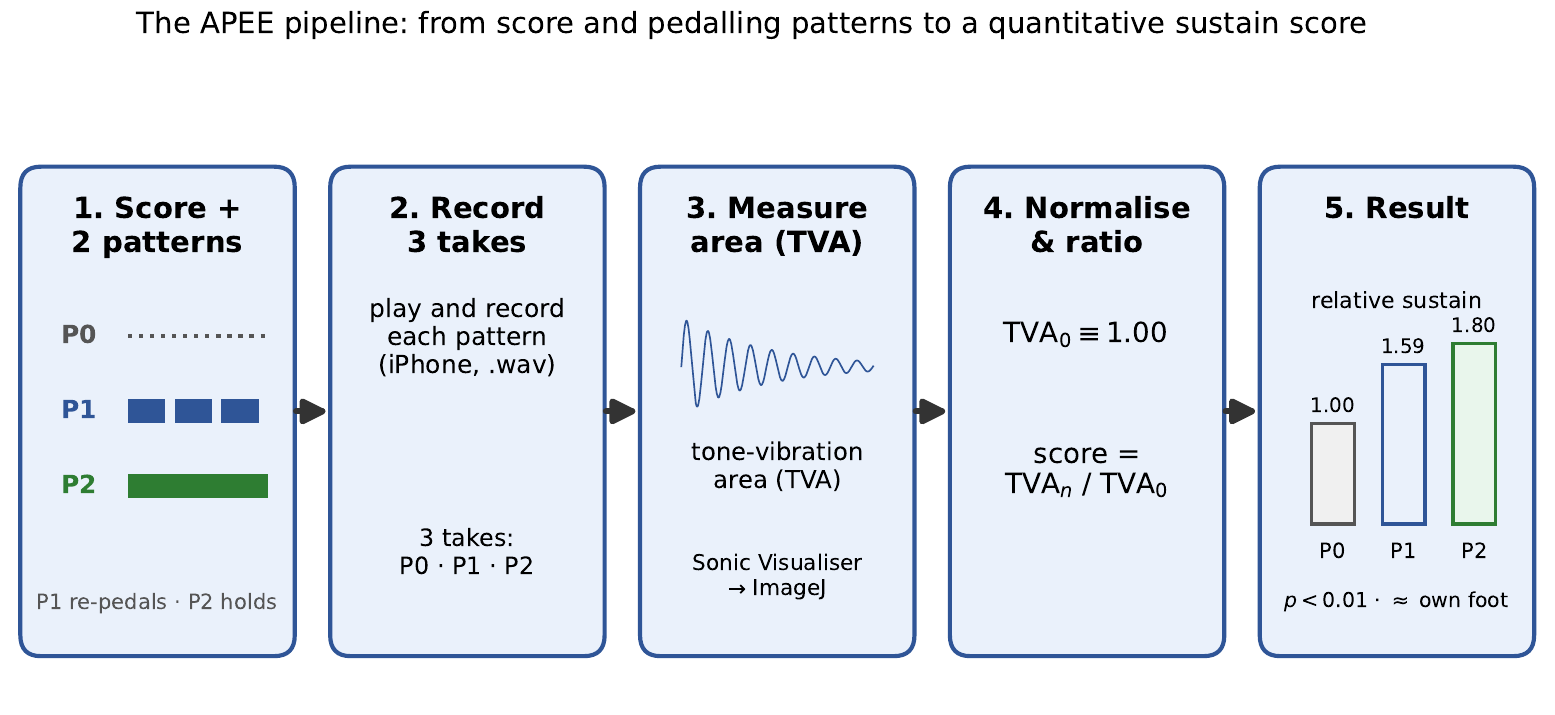
We ran a human-subject study — the Auxiliary Pedal Effect Evaluation (APEE) — with 15 participants: adults, children whose feet don’t reach the pedals, and people with disabilities.

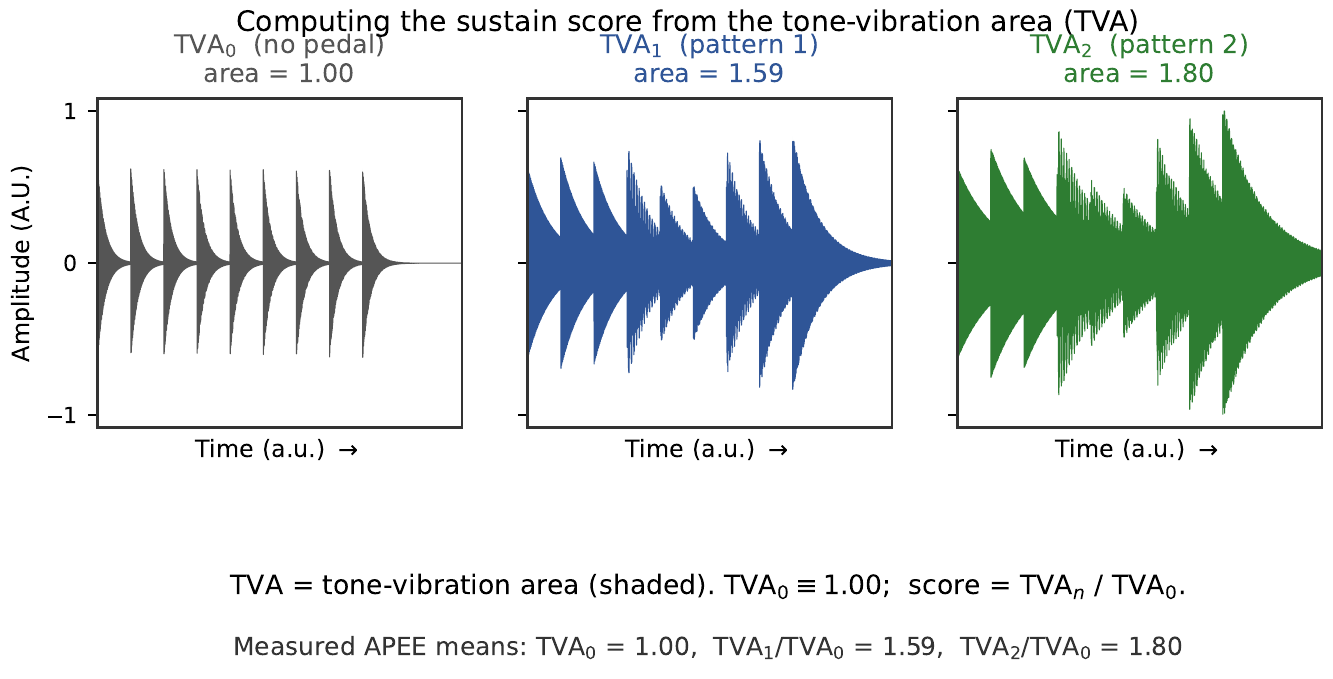
How we measured it
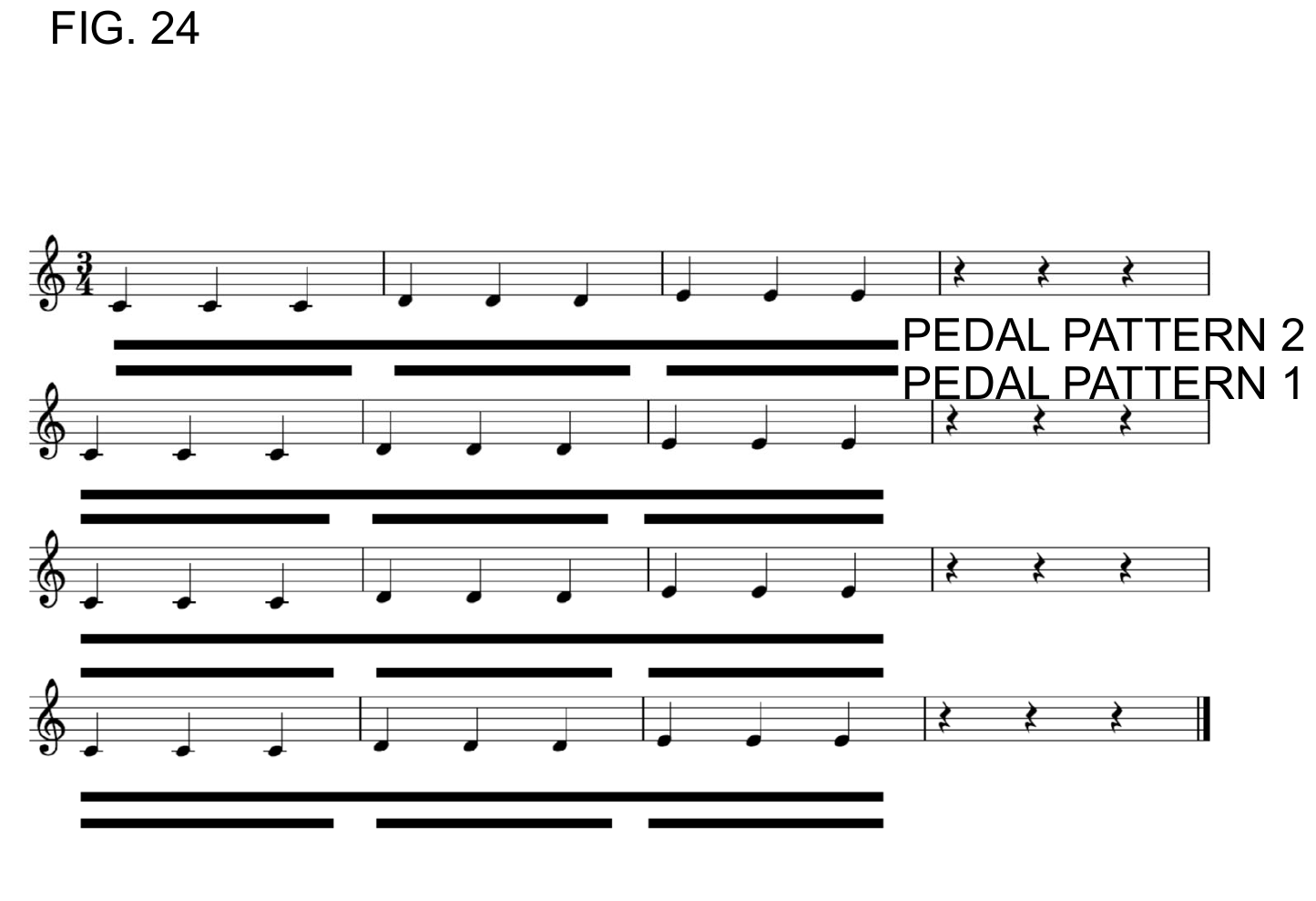
Each participant played the same short motif three ways — no pedal, bFaaaP pattern 1 (re-pedal each three-note group) and pattern 2 (held across groups) — and we recorded each take. We measured the tone-vibration area (TVA), the shaded area of the waveform, and normalized every recording to its own no-pedal take (TVA₀ ≡ 1.00). Sustain score = TVAₙ / TVA₀.
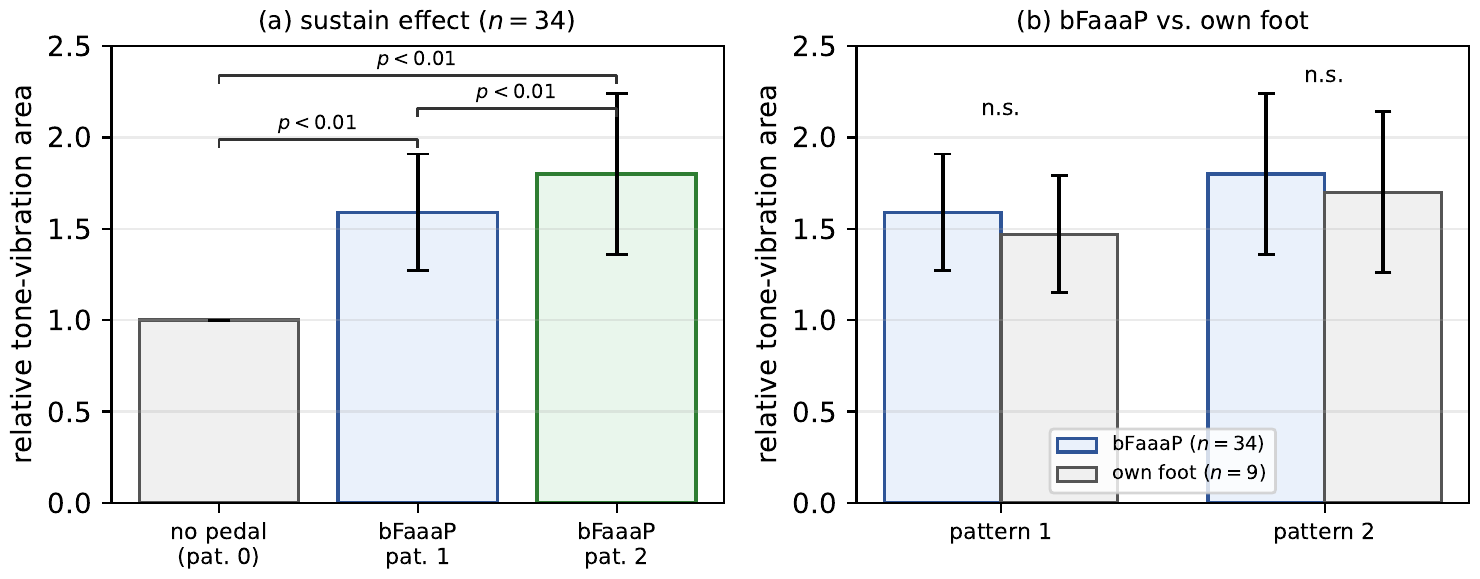
What we found
- bFaaaP significantly increases sustained-tone energy — both patterns beat no pedal (p < 0.01).
- It is statistically indistinguishable from the player’s own foot (p > 0.05, “n.s.”).
- No significant difference across participant classes. One participant with a leg disability and a tracheostomy performed successfully.
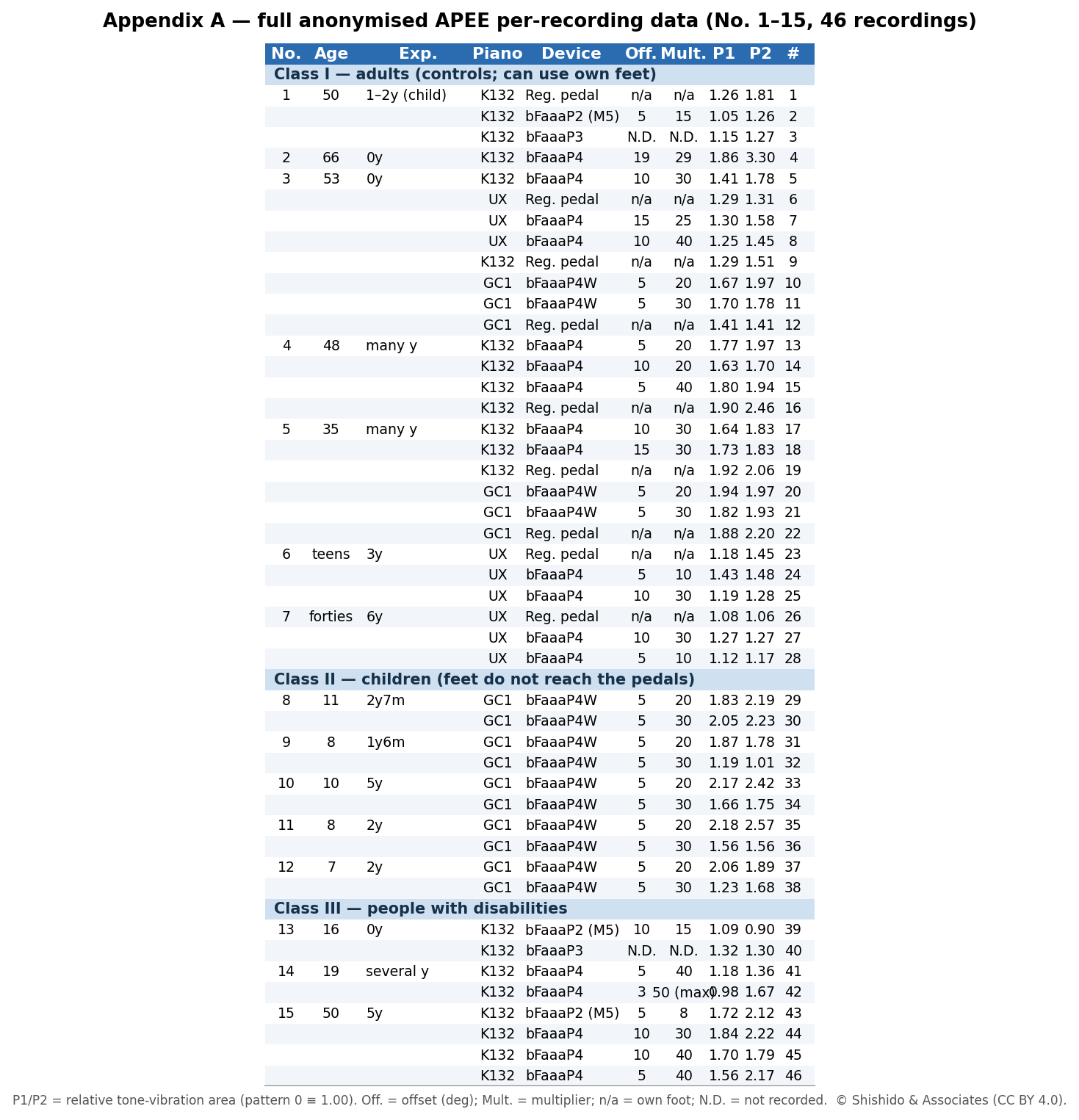
The full anonymized data (Appendix A)
All 46 recordings, participants anonymized as No. 1–15, with each player’s chosen offset and multiplier and the relative sustain of patterns 1 and 2.
Ethics & consent
Participation was voluntary, and written informed consent was obtained for every participant: adults consented themselves; the children signed after a parent or guardian confirmed consent through their piano teacher; and participants with disabilities took part with a parent or guardian’s consent, who also accompanied them. No formal ethics-board (IRB) approval was available, but the study followed the ACM policy on research with human participants, and all data are anonymized.
Ethics & consent on GitHub ↗The controller as a reusable accessibility input
bFaaaP’s smartphone controller — a quantitative, user-tunable head-angle channel on commodity hardware — is the most reusable part. The same controller already drives two actuators (a motor on the Pro, an electronic switch on the Switch), and the device-controller method is patented independently of the pedal, covering “any device.”
- Foot-free — it doesn’t need the lower limbs that wheelchair users often can’t use.
- Nothing on the face or head — the phone sits on a stand (important with a tracheostomy).
- Tunable to a restricted range of motion — a small offset with a large multiplier lets a few degrees of head movement span the full output.
Because the head-angle signal is a continuous, proportional value (not a single on/off switch), it is a general accessibility-control primitive: the same channel could meter other graded controls (environmental control, a communication-aid scan rate, a powered-device level). We present this as future work — bFaaaP is validated for piano pedalling; broader assistive control is not yet validated.
These populations are large and worldwide. The figures below come from heterogeneous surveys with different definitions/metrics and are not strictly comparable — they convey scale, not a ranking. (WHO gives only a single global wheelchair estimate, not a country-by-country table.)
Wheelchair users (or people who need a wheelchair), by region
| Region | Estimate | Source |
|---|---|---|
| World | ~80 million (~1%) need a wheelchair | WHO |
| USA | 3.6 million users (1.5%, 15+), 2010 | US Census |
| UK (England) | ~1.2 million users (est.), 2017 | NHS England |
| Canada | 288,800 wheelchair/scooter users (~1%), 2012 | Smith et al. |
| Japan | ~818,000 manual wheelchairs in use (~0.6%), 2019 | Shirogane et al. |
| Australia | ~119,000 manual users (65+); 679,000 mobility-aid users, 2018 | AIHW/ABS |
Home mechanical ventilation (HMV) & invasive subset, by country
| Country | HMV | Invasive | /100k | Source |
|---|---|---|---|---|
| Japan | ~21,000 | 7,700 (TPPV) | — | MHLW 2020 |
| Europe (16) | 21,526 | varies | 6.6 | Eurovent 2005 |
| Canada | 4,334 | ~18% | 12.9 | Rose 2015 |
| Poland | 12,616 | — | 2.8→20 | JCM 2022 |
| Hungary | 384 | 40 (10.4%) | 3.9 | BMC 2018 |
| South Korea | — | 62.8% trach. | 9.3 | Resp. Care 2019 |
| Germany | ~17,000/yr* | ~6% | — | Dtsch. Ärztebl. 2021 |
| USA | no registry | — | — | Mehta 2015 |
Metrics differ and are not strictly comparable. *inpatient episodes/year; USA has no national home-ventilation registry.
Cited works
Verified June 2026. Full list and saved copies are in the open-source repository.
- WHO. WHO releases new wheelchair provision guidelines. 2023. link
- WHO & UNICEF. Global Report on Assistive Technology. 2022. link
- Brault M. Americans With Disabilities: 2010. US Census Bureau P70-131, 2012. link
- NHS England. Wheelchair services. link
- Smith EM, et al. Prevalence of Wheelchair and Scooter Use Among Community-Dwelling Canadians. Phys Ther 96(8):1135, 2016. link
- Shirogane S, et al. Provision of public funding for wheelchairs… in Japan. J Phys Ther Sci 31(2):122, 2019. link
- AIHW. People with disability in Australia (ABS SDAC 2018). link
- MHLW (Japan). Nationwide home mechanical-ventilation survey (2020). link
- Lloyd-Owen SJ, et al. Patterns of home mechanical ventilation use in Europe (Eurovent). Eur Respir J 25(6):1025, 2005. link
- Rose L, et al. Home Mechanical Ventilation in Canada: A National Survey. Respir Care 60(5):695, 2015. link
- Czajkowska-Malinowska M, et al. Home Mechanical Ventilation in Poland 2009–2019. J Clin Med 11(8):2098, 2022. link
- Valkó L, et al. National survey: home mechanical ventilation in Hungary. BMC Pulm Med 18:190, 2018. link
- Kim H-I, et al. Home Mechanical Ventilation Use in South Korea. Respir Care 64(5):528, 2019. link
- Schwarz SB, et al. Inpatient Initiation and Follow-up of Home Mechanical Ventilation in Germany. Dtsch Arztebl Int 118(23):403, 2021. link
- Mehta AB, et al. Trends in Tracheostomy for Ventilated Patients in the US, 1993–2012. Am J Respir Crit Care Med 192(4):446, 2015. link
- bFaaaP device-controller patent JP 7004771 B2 (covers “any device”). link